Mostly basics
Male: BP occasionally, vaccines, STI testing if risk, mental health/substance use, family history.
Female: BP occasionally, cervical screening by local rules, contraception/pregnancy planning if relevant, vaccines, STI testing if risk.

Useful tests, sensible follow-up
A practical guide to tests by age, sex, family history, symptoms, and risk: fasting, cost, risk, time off work, what each test measures, broad normal ranges, false abnormal results, and the next step if something is not right.
Highest-yield prevention
Worldwide, cardiovascular disease still causes more deaths than any cancer group. The useful midlife move is not one dramatic scan; it is BP, lipids, diabetes risk, smoking, kidney function, weight/waist, symptoms, and family history in one joined-up review.
Languages
Use the selector to open this whole site through Google Translate. The English button always returns to the original page if a translated version becomes hard to navigate.
Principles
A yearly preventive visit is common in the United States and can be useful: it keeps a doctor-patient relationship alive, checks blood pressure, updates medicines and vaccines, and creates space for symptoms people might otherwise ignore. But there are 190-plus other countries, and preventive care has to respect local screening programs, costs, access, ancestry, infectious disease patterns, occupational exposures, and health-system reality. The weaker part everywhere is the automatic "full panel" or full-body scan in healthy people every year.
A better model is simple: use age-appropriate checkpoints at 20, 30, 40, 50, 60, 70 and beyond; check blood pressure more often; use targeted blood tests when risk, age, medicines, symptoms, or prior results justify them; and treat real problems properly when found.
Use the cards below to weigh the pros and cons of routine use without symptoms, understand likely cost and inconvenience, and know what a sensible next step usually looks like. Local costs and normal ranges vary by country, laboratory, insurance, and public health program.
Mild or borderline abnormalities are common. Many need repeat testing, better preparation, or context from symptoms, medicines, alcohol, exercise, hydration, infection, and lab variation before anyone should assume disease.
Otherwise healthy examples
These examples are deliberately conservative. Symptoms, obesity, high BP, smoking, pregnancy history, medicines, alcohol, family history, inherited cancer risk, and inherited lipid disorders can move tests earlier.
Male: BP occasionally, vaccines, STI testing if risk, mental health/substance use, family history.
Female: BP occasionally, cervical screening by local rules, contraception/pregnancy planning if relevant, vaccines, STI testing if risk.
Male: BP, lipids/A1C if family history, obesity, high BP, symptoms, or strong risk.
Female: BP, cervical screening, A1C if gestational diabetes/PCOS/family history/obesity, pregnancy-risk review if relevant.
Male: BP, lipids, A1C/glucose if risk, colorectal plan by 45, earlier with family history or symptoms.
Female: BP, lipids, A1C/glucose if risk, mammogram discussion from 40, colorectal plan by 45.
Male: BP, lipids, cardiovascular risk score, A1C/glucose, creatinine/eGFR, colorectal screening, PSA informed choice, vaccines.
Female: BP, lipids, A1C/glucose, creatinine/eGFR, colorectal screening, mammogram, cervical screening if still due, vaccines.
Male: manage BP/lipids/diabetes, colorectal screening, PSA informed choice, lung CT if eligible, eye/hearing/bone risk.
Female: manage BP/lipids/diabetes, mammogram/colorectal screening, bone-risk review, eye/hearing checks.
All: medicines, falls, BP without overtreatment, kidney/electrolytes if on relevant drugs, vision, hearing, cognition, mood, goals of care.
Cancer screening depends on health, previous screening, preferences, and whether an abnormal result would lead to wanted treatment.
Before booking tests
BP is worth checking often. Lipids are cardiovascular risk factors, not a disease by themselves. Cholesterol pattern, A1C/glucose, creatinine/eGFR, and blood count may be worth at least a baseline around midlife, then repeats depend on risk and findings.
Fevers, weight loss, bleeding, chest pain, lumps, fainting, night sweats, or new neurological symptoms are diagnostic problems, not routine screening problems.
A useful test has a follow-up path: repeat, confirm, image, biopsy, treat, monitor, or refer. If no action would follow, ask why it is being done.
The test guide
Use the filters to narrow the list. Normal ranges below are broad guideposts, not personal targets. Your lab report and clinician's advice matter most.
What waiting can look like
These images are deliberately direct. They are educational examples, not interpretations of any individual person's scan or wound. The lesson is simple: cancer, bleeding, eye disease, and organ problems often do not announce themselves early. The right test at the right time can turn a late emergency into a planned procedure.
A suspicious skin lesion does not "pop out" neatly by itself. A bowel cancer does not wait until your calendar is convenient. A scan can become necessary because a quiet abnormality was ignored. Prevention is not about ordering every test; it is about not wasting the tests that actually change outcomes.
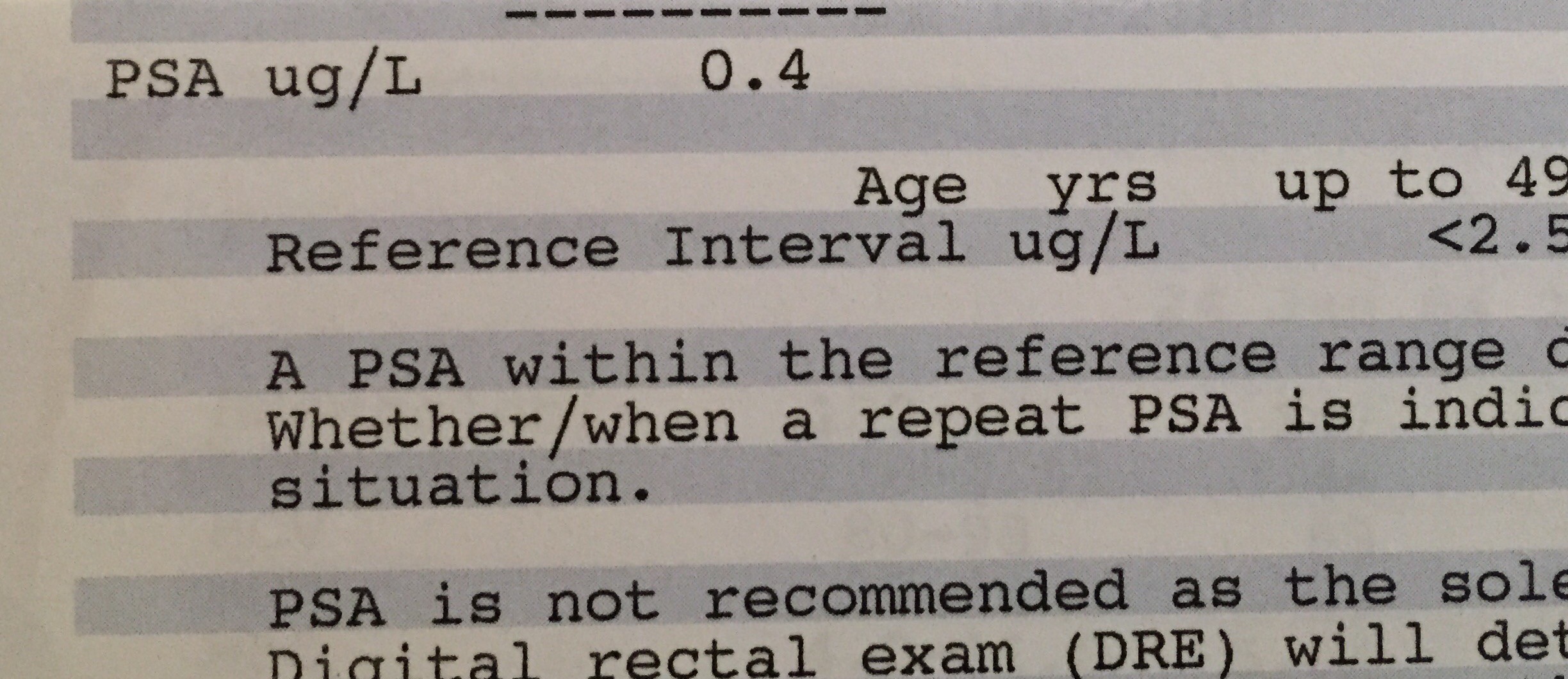
PSA is best interpreted by age, prostate size, family history, infection risk, medications, and trend. A single number is not a diagnosis, but it can guide sensible follow-up.

High LDL is not a heart attack, but it is a risk factor worth confirming and treating with the full picture: family history, BP, diabetes, smoking, weight, diet, exercise, and medication options.
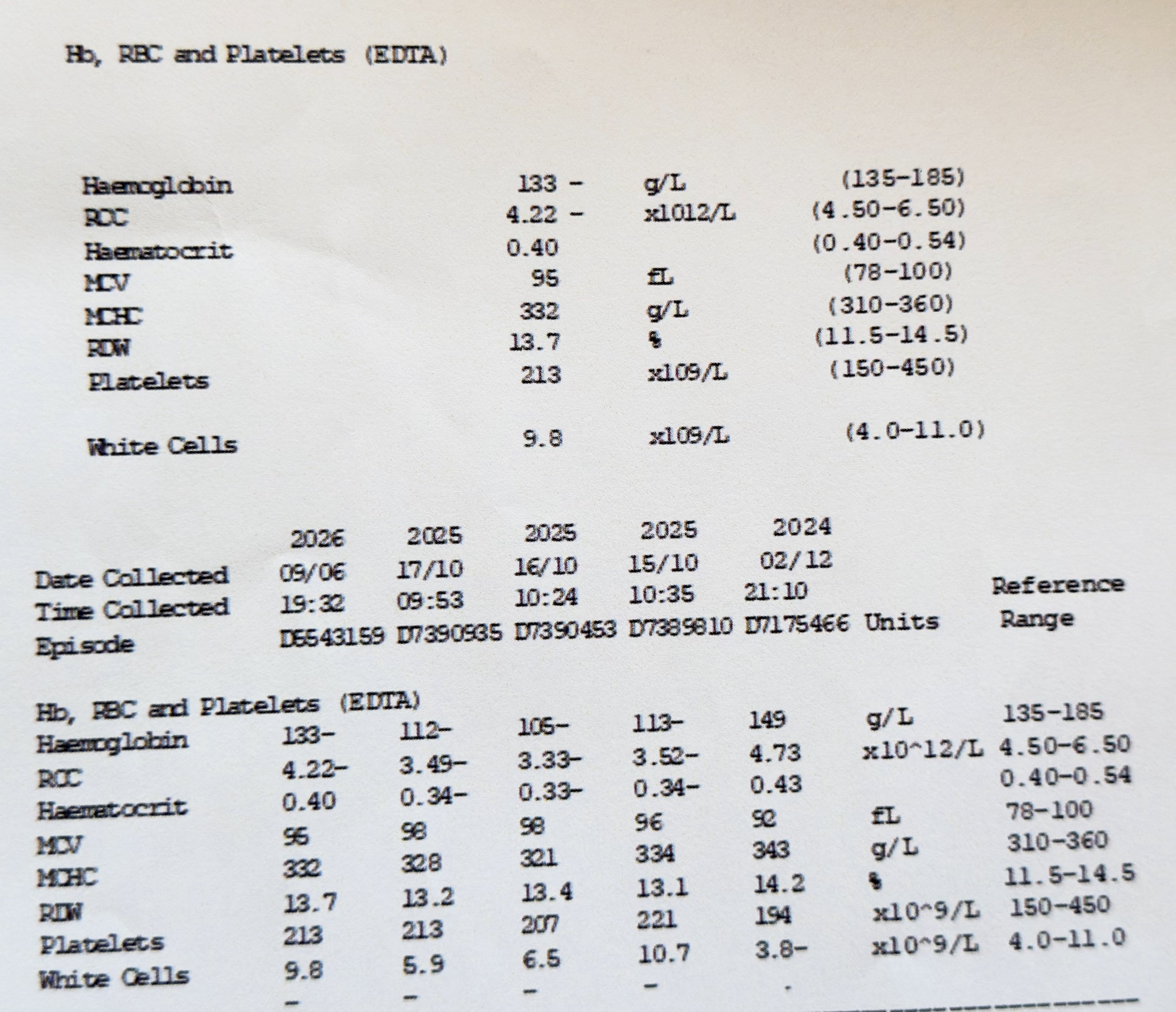
Hemoglobin, red cells, platelets, and white cells can reveal anemia, inflammation, infection patterns, medication effects, or blood disorders. Mild changes often need repeat testing rather than panic.
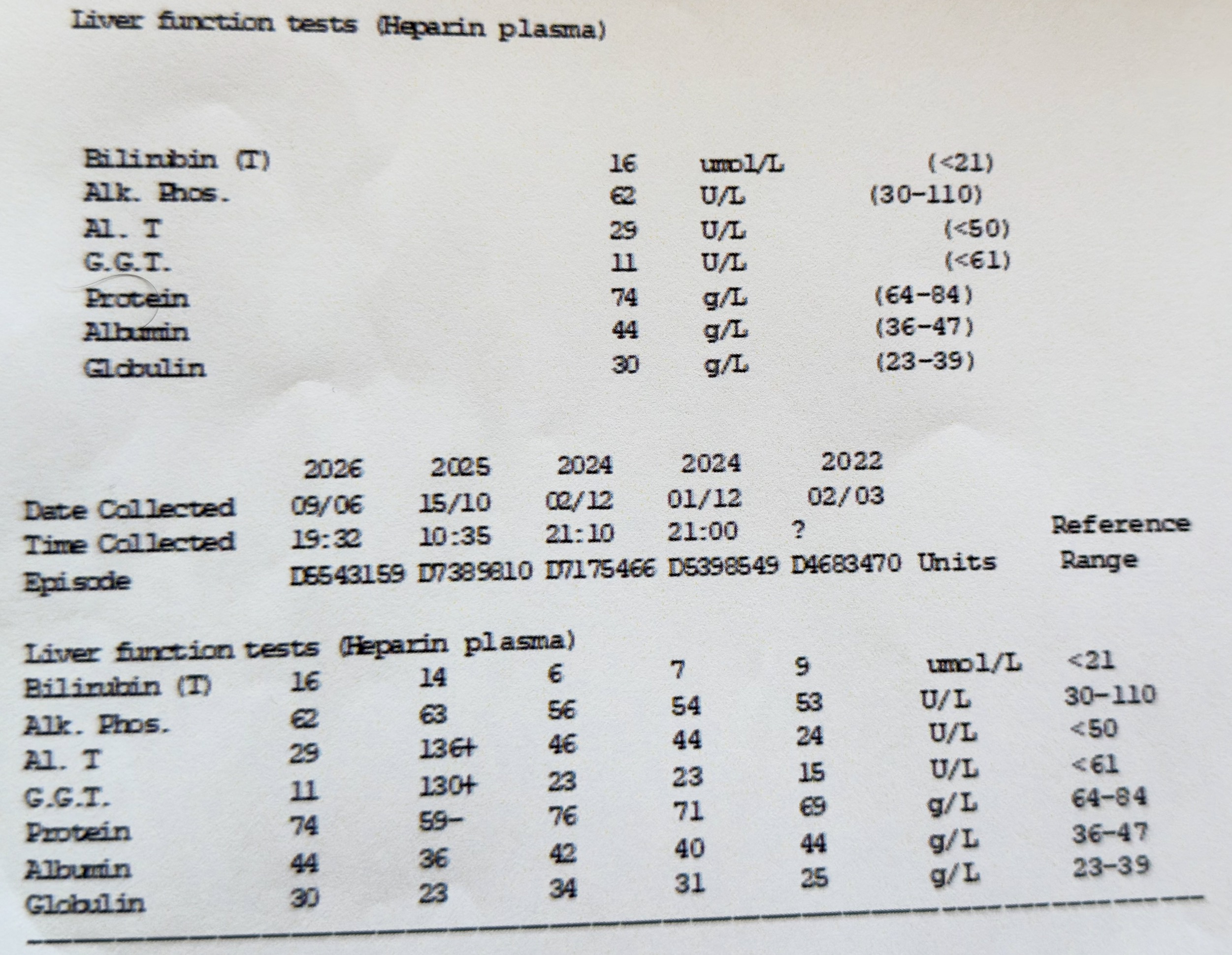
Bilirubin, ALP, ALT, GGT, protein, albumin, and globulin are interpreted with alcohol, weight, viral risk, medicines, supplements, symptoms, and prior results.
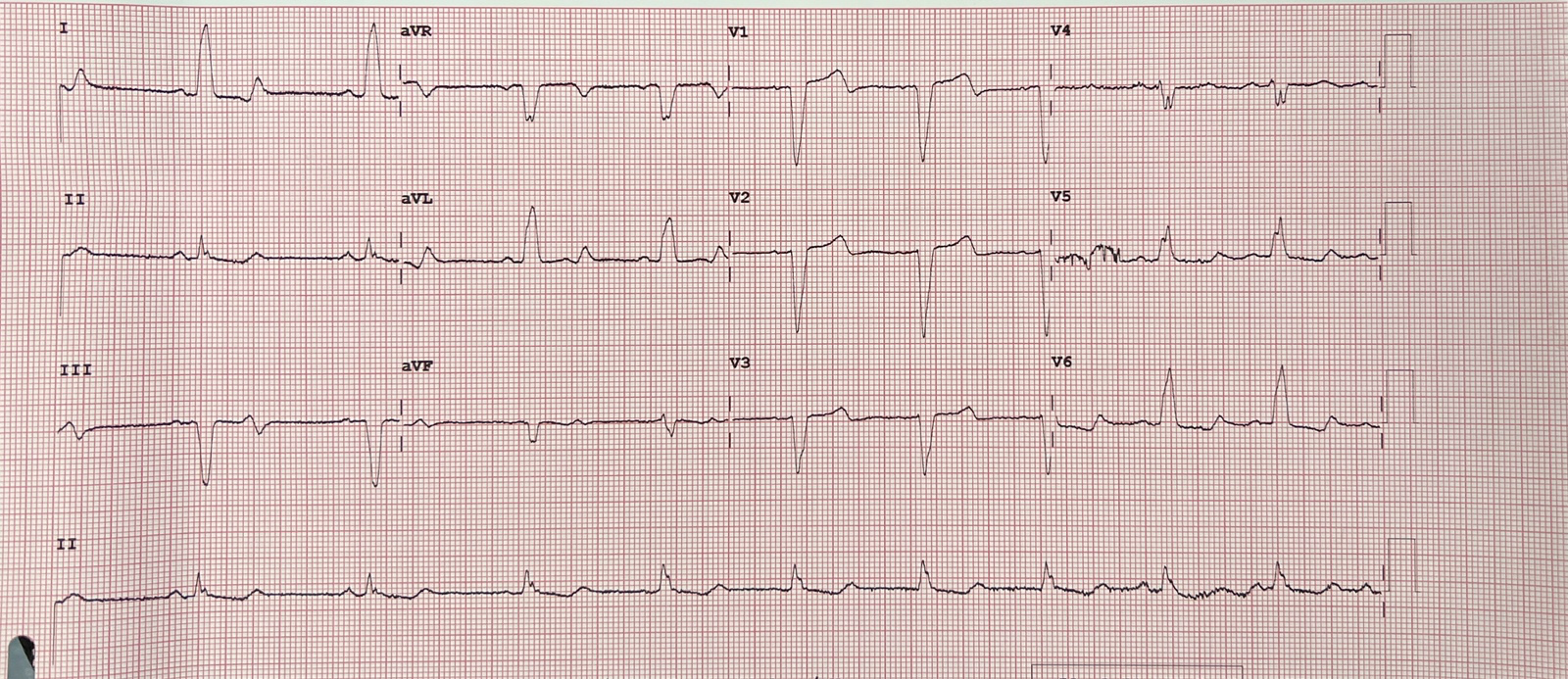
An abnormal ECG needs clinical context: symptoms, old ECGs, medications, electrolytes, blood tests, and whether the change is new. Chest pain, fainting, or breathlessness changes urgency.

Suspicious skin cancers are cut out with a margin of normal-looking skin. Earlier detection can mean a smaller excision, clearer planning, and less tissue removed.

The face is not a place to gamble with a changing spot. Early assessment can mean a planned local procedure rather than a larger reconstruction later.

Scalp, ear, nose, lip, and neck lesions are easy to miss. A proper skin check includes hidden sun-exposed areas, not only obvious moles.

Surgeons remove the visible lesion plus a safety margin. On the nose, even a modest cancer can leave a defect that needs careful repair.
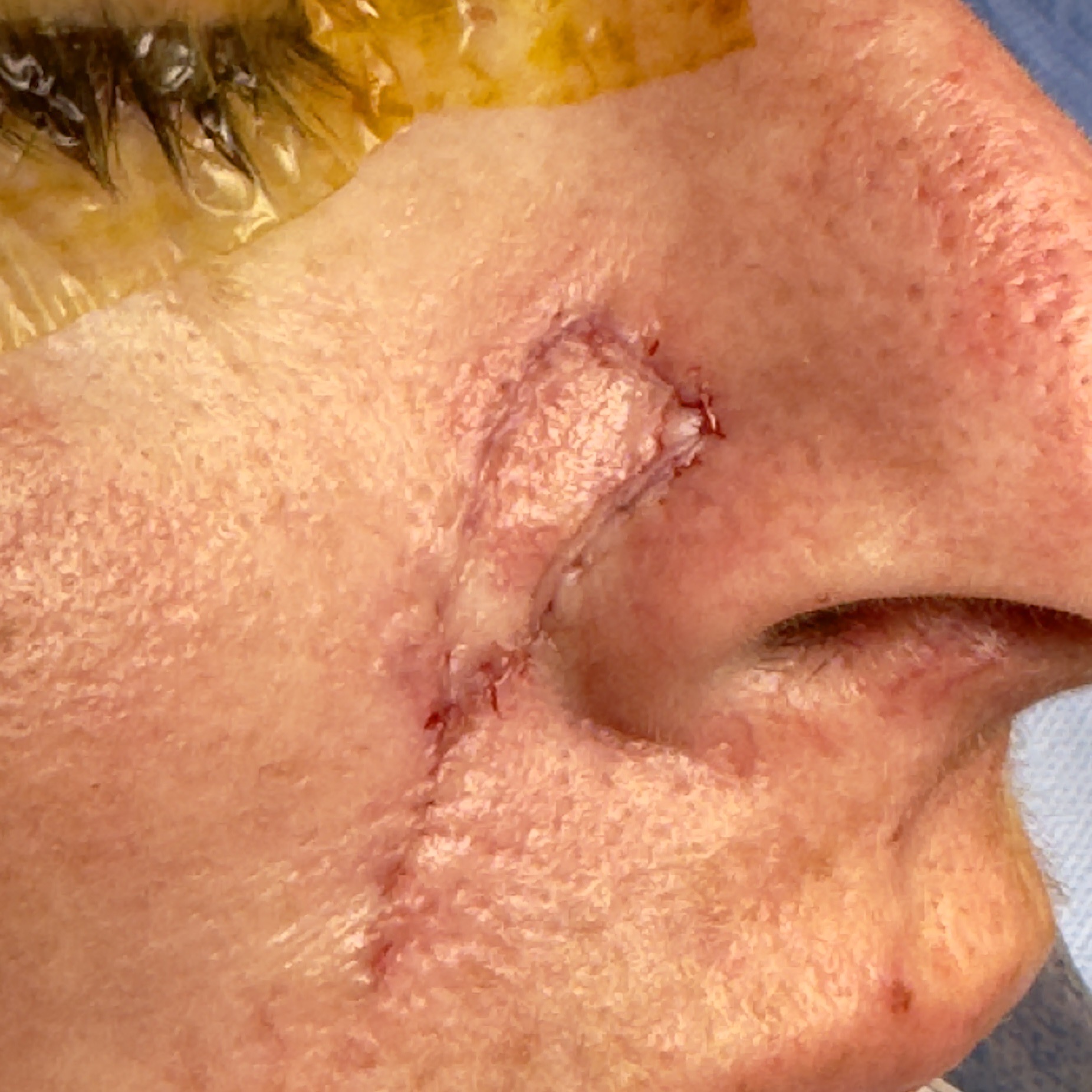
The neat scar people hope for depends on early diagnosis, complete removal, margin control, wound planning, and follow-up. It is not magic after months of waiting.

Surgeons shape and close wounds to reduce tension and minimize scarring, but waiting can make the operation larger than it needed to be.
FIT screening and colonoscopy exist because early bowel cancer and dangerous polyps may cause no pain. Blood in stool, iron deficiency, weight loss, or bowel change should not be shrugged off.

Colonoscopy can biopsy suspicious lesions and remove many polyps before they become cancer. Repeating a positive FIT instead of investigating it can lose precious time.
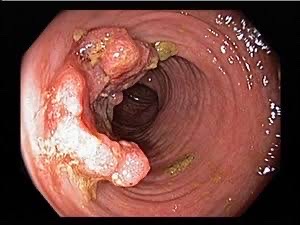
Many polyps are benign, but pathology determines risk. The practical win is that screening can find problems while they are still treatable or removable.
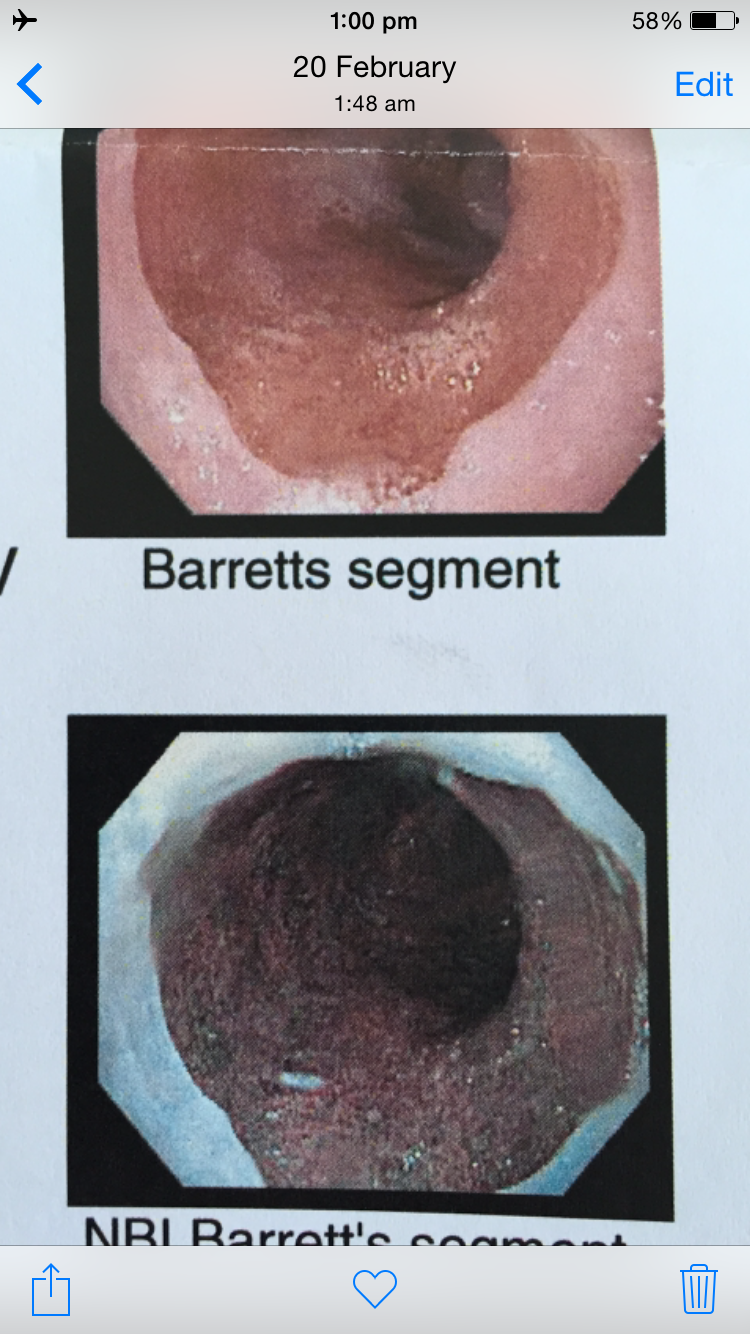
Most heartburn is not cancer, but swallowing trouble, bleeding, unexplained iron deficiency, weight loss, or Barrett's risk changes the conversation.
See refluxsurgery.com for Barrett's and reflux surgery context.
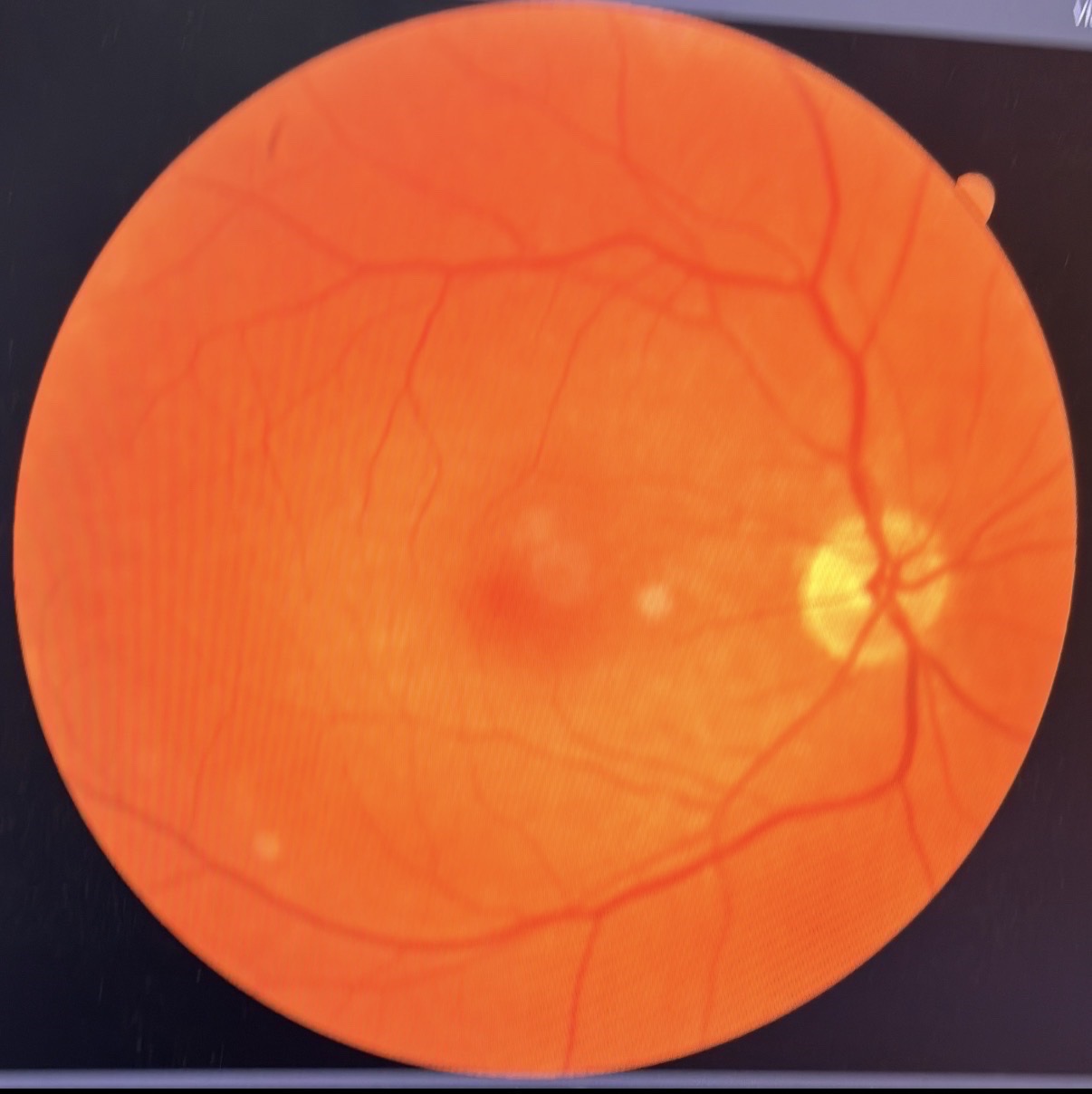
Diabetes, high blood pressure, glaucoma risk, and retinal disease can progress before vision feels wrong. Eye checks are not vanity; they are vascular screening with a lens.

PET-CT can stage or investigate cancer, but it brings radiation, cost, false positives, and incidental findings. It should answer a real clinical question.
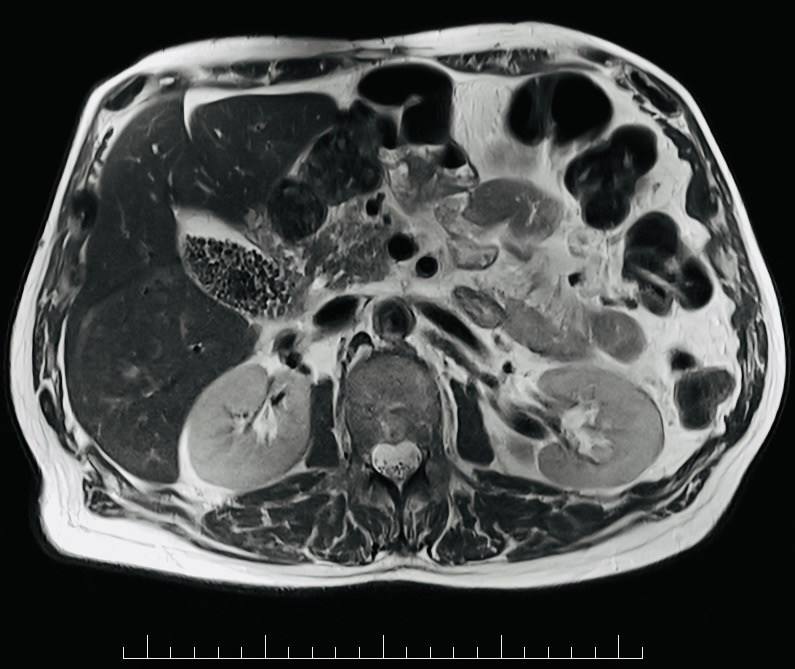
MRI is excellent for selected questions. It can also reveal incidental cysts, disc changes, or benign findings that create worry unless interpreted in context.

Images can look dramatic to non-radiologists. Decisions should come from the written report, symptoms, prior scans, blood tests, and the specialist's plan.
Cancer map
This is the part people often get wrong. A good screening test is not just a test that can find cancer; it must find it early enough, often enough, and safely enough to improve outcomes. For several frightening cancers, routine screening in average-risk people is not proven. That makes symptoms and family history even more important.
Useful checks: self-checks, clinician skin exam, dermoscopy, mole photography when high risk.
Act on: changing, bleeding, non-healing, asymmetrical, black/blue, crusting, tender, or rapidly growing spots.
Next step: urgent dermoscopy or biopsy. If cancer, excision with margins; earlier usually means less tissue removed.
Useful checks: FIT/FOBT screening and colonoscopy from guideline age, earlier with family history or symptoms.
Act on: rectal bleeding, iron deficiency, black stools, bowel habit change, weight loss, abdominal mass, persistent pain.
Next step: positive FIT or concerning symptoms usually need colonoscopy, biopsy, pathology, and interval planning.
Useful checks: exam, anoscopy/high-resolution anoscopy, anal cytology in selected high-risk groups.
Act on: bleeding, pain, lump, ulcer, discharge, HPV-related disease, immune suppression, or persistent symptoms.
Next step: exam, swab/biopsy, colorectal or sexual-health specialist review.
Useful checks: PSA after informed discussion, especially around 50-69; earlier with strong family history or high-risk ancestry.
Act on: rising PSA trend, abnormal exam, bone pain, blood in urine, urinary symptoms with risk, or family history. Early prostate cancer may have no symptoms and a normal-sized prostate.
Next step: repeat PSA, urine test, risk calculator, prostate MRI, urology review, biopsy if risk remains concerning.
Useful checks: mammography by age/risk; MRI for selected high-risk genetic/family-history groups.
Act on: new lump, nipple inversion/discharge, skin dimpling, bloody discharge, persistent focal pain, armpit lump.
Next step: diagnostic mammogram, ultrasound, MRI if indicated, and image-guided biopsy for suspicious findings.
Useful checks: genetic risk assessment for BRCA/Lynch patterns; specialist surveillance only for selected high-risk people.
Act on: persistent bloating, early fullness, pelvic pain, urinary frequency, weight loss, new abdominal swelling.
Next step: pelvic exam, transvaginal ultrasound, CA-125 in context, CT, gynecology/oncology review. CA-125 alone is not a simple screening answer.
Useful checks: cervical HPV/Pap screening prevents cervical cancer. There is no routine endometrial cancer screen for average-risk people.
Act on: bleeding after menopause, bleeding between periods, heavy new bleeding, pelvic pain, abnormal cervical screening.
Next step: cervical follow-up/colposcopy for HPV/Pap changes; pelvic ultrasound and endometrial biopsy for post-menopausal bleeding.
Useful checks: self-awareness and prompt exam; routine formal screening is not generally recommended for average-risk men.
Act on: painless lump, swelling, heaviness, firmness, ache, size change, or history of undescended testis.
Next step: urgent ultrasound, tumor markers, urology referral. Do not wait for pain.
Useful checks: genetic/family-history review; MRI/EUS surveillance only in selected high-risk families or syndromes such as strong familial pancreatic cancer patterns, BRCA/Lynch/PALB2/ATM with affected relatives, Peutz-Jeghers, CDKN2A, or hereditary pancreatitis.
Act on: painless jaundice, dark urine, pale stools, new diabetes with weight loss, persistent upper abdominal/back pain, unexplained weight loss.
Next step: liver tests, CT pancreas protocol or MRI/MRCP, CA19-9 in context, endoscopic ultrasound/biopsy, specialist referral.
Useful checks: neck exam and ultrasound for a real nodule. Routine ultrasound screening can find tiny cancers that never cause harm.
Act on: growing neck lump, hoarseness, swallowing trouble, radiation exposure history, suspicious lymph nodes.
Next step: TSH, ultrasound risk scoring, fine-needle biopsy if indicated, endocrine/surgical review.
Useful checks: dental/oral exam, especially with tobacco, alcohol, HPV risk, poor dentition, or persistent lesions.
Act on: ulcer over 2-3 weeks, red/white patch, lump, loose teeth, one-sided throat pain, voice change, neck node.
Next step: dentist/ENT review, flexible nasendoscopy, biopsy, imaging if suspicious.
Useful checks: H. pylori testing/treatment when indicated, gastroscopy for alarm symptoms or Barrett's surveillance.
Act on: swallowing trouble, food sticking, vomiting blood, black stools, iron deficiency, weight loss, persistent reflux with risk factors.
Next step: gastroscopy with biopsy, H. pylori treatment, CT/EUS staging if cancer is found.
Useful checks: low-dose CT for eligible smoking-history groups; specialist advice may be needed when asbestos, silica, radon, diesel, COPD, pulmonary fibrosis, or family history changes risk. Chest X-ray is not a reliable screening substitute.
Act on: coughing blood, persistent cough, weight loss, chest pain, breathlessness, recurrent pneumonia, hoarseness.
Next step: chest X-ray for symptoms when appropriate, CT, PET-CT, bronchoscopy or needle biopsy, respiratory and oncology review.
Useful checks: no routine screen for average-risk adults; ultrasound/CT when symptoms or inherited risk justify it.
Act on: blood in urine, flank pain, abdominal mass, unexplained anemia, fevers, weight loss, high-risk syndromes.
Next step: urinalysis, kidney function, ultrasound or CT, urology review.
Useful checks: ultrasound with or without AFP every 6 months for cirrhosis or selected chronic hepatitis B risk groups.
Act on: known cirrhosis, hepatitis B/C, heavy alcohol liver disease, fatty liver with advanced fibrosis, weight loss, jaundice, swelling.
Next step: liver ultrasound, AFP, contrast CT/MRI liver protocol, hepatology review, antiviral/alcohol/metabolic treatment.
The big age-related issues
Cancer gets attention, but heart disease, stroke, diabetes, kidney disease, dementia, falls, frailty, alcohol harm, depression, and sleep apnea often do more total damage. The goal is not a perfect lab sheet. The goal is staying alive, mobile, independent, and mentally present.
Useful checks: blood pressure, lipid profile, formal cardiovascular risk score, A1C/glucose, kidney function, smoking status, weight/waist, family history, ECG if symptoms or risk.
Do not ignore: chest pressure, exertional breathlessness, fainting, fast or many missed heartbeats, one-sided weakness, speech trouble, new severe headache.
Action: treat confirmed high BP, statins when risk justifies, diabetes care, smoking cessation, exercise, sleep apnea treatment, cardiology review when symptoms/risk justify it, urgent stroke/chest-pain pathways.
Useful checks: A1C or fasting glucose, BP, lipids, kidney function, urine albumin, eye exam, foot checks if diabetes is present.
Do not ignore: thirst, urination, blurred vision, recurrent infections, numb feet, fatigue, obesity, family history, prior gestational diabetes or PCOS.
Action: obesity treatment, resistance/aerobic exercise, nutrition, sleep, GLP-1/SGLT2/metformin/insulin when indicated, retinal and kidney protection.
Useful checks: BP, diabetes risk, lipids, smoking, atrial fibrillation clues, alcohol, sleep apnea, mood, medicines, hearing/vision, B12/thyroid when indicated, and cognitive testing when concerns arise.
Do not ignore: one-sided weakness, speech trouble, sudden confusion, stepwise decline after small strokes, getting lost, financial mistakes, repeated falls, personality change, hallucinations, unsafe driving, heavy alcohol use, or new severe headache.
Action: urgent stroke pathways for sudden symptoms, treat BP/diabetes/lipids/atrial fibrillation, reduce alcohol harm, protect hearing and sleep, review sedatives, support carers, driving/work safety, advance planning, memory clinic referral when needed. Dementia is not just Alzheimer's; vascular, multi-infarct, alcohol-related, medication-related, mood/sleep-related, Parkinson's/Lewy body, and mixed patterns all change the work-up.
Useful checks: creatinine/eGFR, urine albumin, BP, diabetes control, medication review, NSAID exposure, ultrasound if persistent abnormalities.
Do not ignore: swelling, foamy urine, blood in urine, uncontrolled BP, worsening diabetes, dehydration with kidney-toxic medicines.
Action: BP control, ACE/ARB/SGLT2 where appropriate, avoid nephrotoxins, treat obstruction, nephrology referral for progressive or severe disease.
Useful checks: falls history, gait/balance, vision, hearing, medicines, vitamin D/calcium context, DXA when fracture risk is meaningful.
Do not ignore: near-falls, dizziness, sedatives, weak legs, previous fracture, weight loss, loneliness, unsafe home setup.
Action: strength and balance training, medicine reduction, home safety, osteoporosis treatment when risk is high, hearing/vision correction.
Useful checks: alcohol history, liver tests when risk/symptoms, hepatitis testing if risk, FibroScan/ultrasound for persistent abnormalities or metabolic risk.
Do not ignore: jaundice, abdominal swelling, vomiting blood, black stools, confusion, unexplained bruising, weight loss.
Action: low or moderate alcohol, alcohol reduction/cessation support when needed, viral hepatitis treatment, weight/metabolic treatment, fibrosis assessment, hepatology referral for advanced disease.
Useful checks: smoking status, alcohol pattern, waist/weight trend, exercise capacity, sleep apnea risk, diet quality, BP response.
Do not ignore: inability to climb stairs, new exercise intolerance, continued smoking, escalating alcohol, central weight gain, or breathlessness.
Action: nicotine replacement at an adequate dose or combination therapy, quit support, 150-300 minutes weekly moderate aerobic activity when possible, resistance training at least twice weekly, and nutrition support.
Useful checks: depression/anxiety screen, alcohol/substance review, sleep apnea risk, medication review, blood pressure and weight context.
Do not ignore: suicidal thoughts, panic, escalating alcohol, severe insomnia, loud snoring with daytime sleepiness, near-miss driving events.
Action: safety plan, therapy, medicines when appropriate, sleep study/CPAP, alcohol treatment, workplace and family support.
Useful checks: hearing screen, eye pressure/retina/glasses, dental review, foot pain, arthritis function, driving safety.
Do not ignore: withdrawal from conversation, missed medication labels, poor night driving, dental infection, foot ulcers, pain limiting walking.
Action: hearing aids, cataract/glaucoma care, dental treatment, podiatry, pain plan, exercise rehab, transport and home adaptations.
Result examples
These are educational examples, not personal medical advice. A clinician should interpret your own results with your age, symptoms, family history, medicines, and prior results.
Prostate cancer awareness campaigns are useful because men often wait for symptoms, and early prostate cancer may cause none. But PSA testing is still a shared decision: useful for some, misleading for others, and best interpreted by age, baseline value, family history, ancestry, urinary symptoms, prostate size, infection risk, and trend.
A real age-50 check found PSA 9 despite no urinary symptoms and a normal-sized prostate. His father had prostate cancer, common but still relevant. Ultrasound and biopsy found medium-grade cancer involving about half the prostate; if left much longer, spread beyond the prostate was a serious concern.
Because it was caught in time, open nerve-sparing radical prostatectomy was possible. Incontinence and impotence were avoided, PSA has stayed zero for more than 23 years, and no radiotherapy or chemotherapy was needed. This does not make PSA mandatory for every man, but it shows why an informed PSA discussion at 50 can matter.
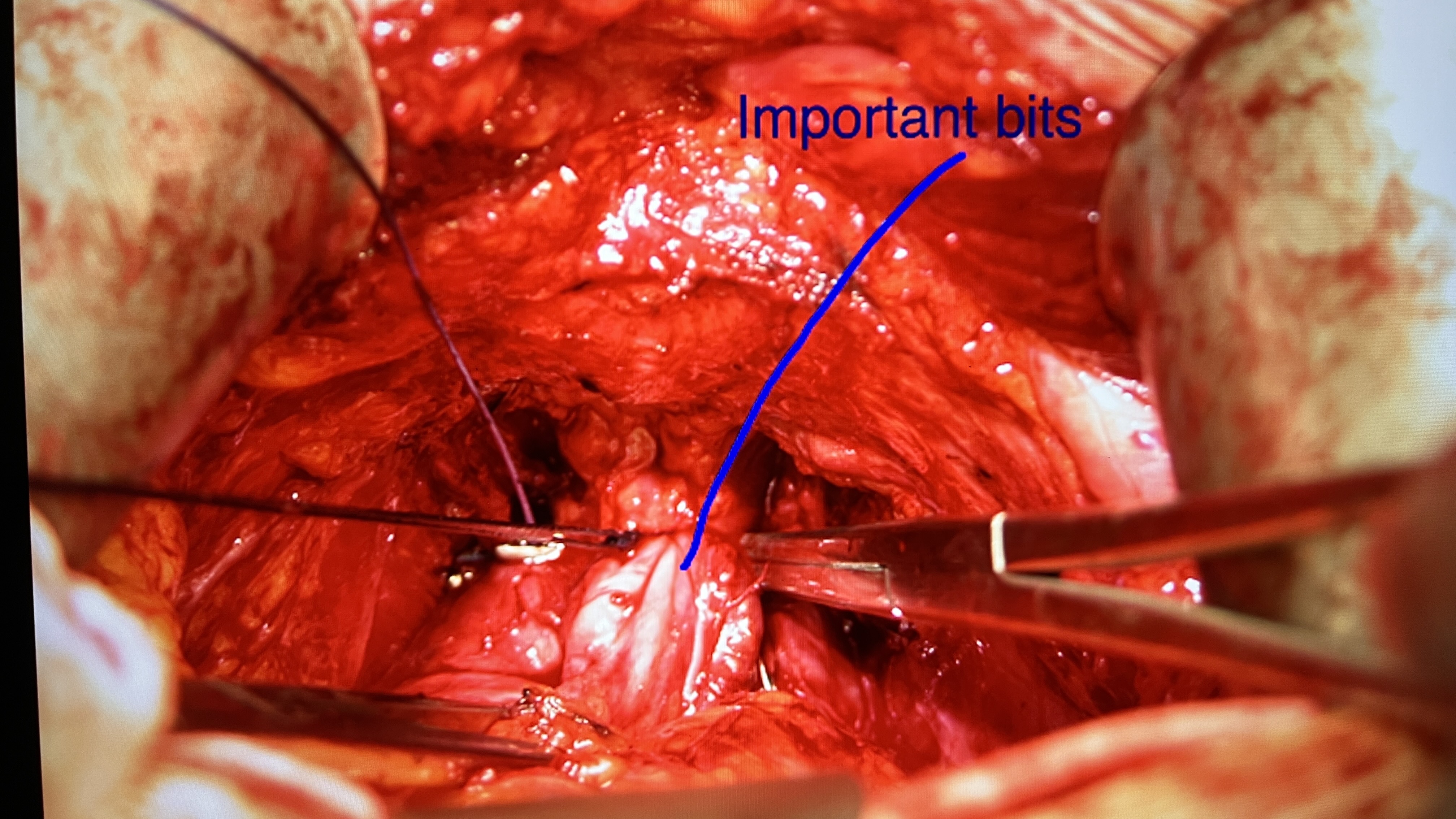
This graphic operative image shows the author's prostate being removed. The practical point is not the photograph itself; it is the window of opportunity. A quiet PSA result led to diagnosis while curative surgery was still possible.
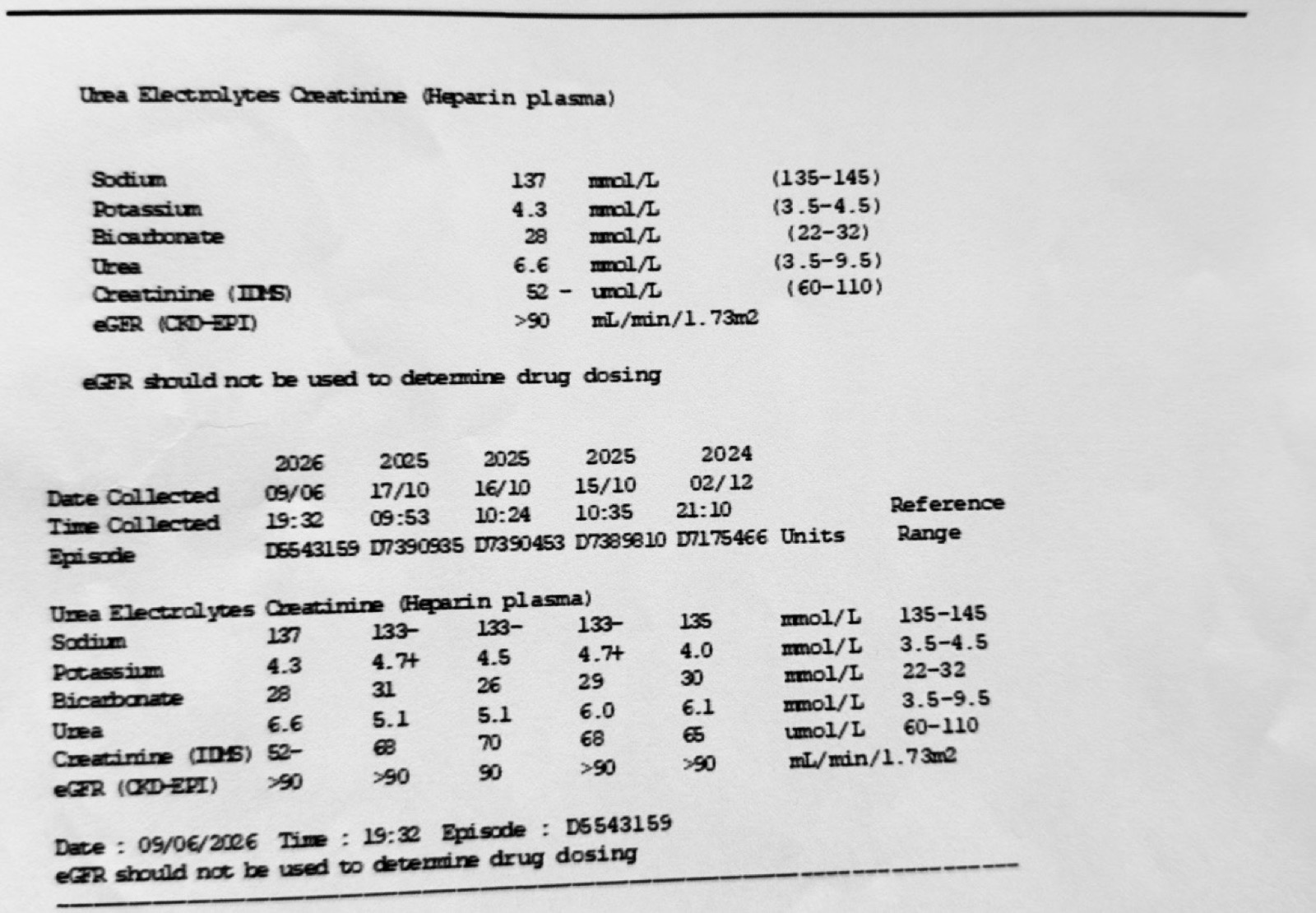
A creatinine and eGFR baseline can be boring in the best possible way. It helps later when a person starts blood pressure medicines, diabetes medicines, anti-inflammatories, contrast scans, or becomes unwell and the clinician needs to know what normal used to look like.
An ECG pattern such as left bundle branch block can be old and stable, or it can matter a lot if it is new, unexplained, or paired with chest pain, breathlessness, fainting, palpitations, or poor exercise tolerance. It usually needs comparison with prior ECGs and clinical assessment rather than machine-text panic.
For example, a PSA around 0.4 ug/L in the early 40s is generally a low baseline. That does not mean "never test again," but it can support a calmer, less frequent follow-up plan unless family history, symptoms, or risk changes.
A lipid result such as total cholesterol 7.8 mmol/L, LDL 5.4 mmol/L, non-HDL 6.5 mmol/L, and triglycerides 2.4 mmol/L is high enough to deserve follow-up. It should usually trigger repeat/confirmation, cardiovascular risk calculation, family-history review, secondary-cause review, and discussion of diet, weight, alcohol, exercise, smoking, statin therapy, or other lipid-lowering treatment.
One de-identified example: hemoglobin 133 g/L, RBC 4.22 x10^12/L, hematocrit 0.40, MCV 95 fL, MCHC 332 g/L, RDW 13.7%, platelets 213 x10^9/L, white cells 9.8 x10^9/L. The hemoglobin and RBC are just below that lab's male reference range, while platelets and total white cells are within range.
Next step is not panic. Consider prior baseline, bleeding, iron/B12/folate, kidney disease, inflammation, alcohol, medicines, recent surgery or illness, and repeat testing if unexpected or persistent.
Example differential: white cells 9.8 x10^9/L, neutrophils 8.0 x10^9/L, lymphocytes 1.3 x10^9/L, monocytes 0.5 x10^9/L, eosinophils 0.0 x10^9/L, basophils 0.1 x10^9/L. Mild neutrophilia with low-ish lymphocytes can occur with acute illness, inflammation, stress response, steroid effect, smoking, or recovery after a procedure.
Trend matters. Persistent, extreme, unexplained, or symptom-linked changes need clinician review rather than isolated interpretation.
Example CRP: current CRP 2.0 mg/L with a reference of less than 5.0, after earlier elevated values above 20-70 mg/L. CRP is a nonspecific inflammation marker; infection, surgery, injury, inflammatory disease, and some cancers can raise it.
A normalizing CRP can be reassuring when the person is clinically improving. A high or rising CRP without a clear reason should be interpreted with symptoms, examination, cultures, imaging, and other blood tests.
Example current liver results: bilirubin 16 umol/L, alkaline phosphatase 62 U/L, ALT 29 U/L, GGT 11 U/L, protein 74 g/L, albumin 44 g/L, globulin 30 g/L. These sit within the displayed reference ranges.
Earlier spikes in ALT or GGT can follow alcohol, fatty liver, viral illness, medicines, supplements, bile-duct problems, muscle injury, or lab timing. The useful response is to repeat, review causes, and investigate persistent or severe abnormalities.
LDL around 5 mmol/L or higher, especially when persistent or combined with early heart disease in relatives, can suggest familial hypercholesterolemia. Next steps may include repeat fasting lipids, ApoB, Lp(a), thyroid and diabetes checks, secondary-cause review, and sometimes genetic testing or cascade testing for relatives.
Lipids can be affected by diet, alcohol, weight, diabetes, thyroid disease, kidney disease, liver disease, pregnancy, medicines, and genetics. PSA can be affected by infection, inflammation, ejaculation, cycling, procedures, prostate size, and cancer. The pattern is the point.
A colon polyp found and removed at 45 may prevent a future cancer, especially when follow-up colonoscopies stay clear. Barrett's esophagus after years of severe GERD/GORD reflux is another example: fundoplication can control reflux for selected people, but Barrett's still needs surveillance even after symptoms improve. See refluxsurgery.com.
Abnormal results
Many results sit just outside the reference range. Reference ranges are usually built so that some healthy people fall outside them. The next step depends on how abnormal the result is, whether it fits your symptoms, whether it was repeated, and whether several related markers point in the same direction.
Cost matters too. A cheap blood test can become expensive if it triggers scans, specialist appointments, or biopsies that do not improve outcomes. That does not mean avoid testing; it means test with a reason and a plan.
Do act quickly for clearly dangerous findings: very high blood pressure with symptoms, severe anemia, very high glucose with illness, chest pain, stroke symptoms, black stools, major bleeding, severe kidney changes, or imaging that is suspicious for cancer.
For mild changes, the sensible path is often repeat, confirm, then treat the actual condition: diabetes, high blood pressure, high cardiovascular risk, cancer, kidney disease, thyroid disease, iron deficiency, depression, sleep apnea, or another defined issue.
When to test
Blood pressure, lipid baseline, diabetes risk, family history, reproductive history where relevant, mental health, vaccines, and symptom-led screening.
Colorectal screening should be current, vaccines follow local rules, and baseline checks such as BP, lipid pattern, cardiovascular risk score, A1C/glucose, creatinine/eGFR, ECG when symptoms/family history/risk justify it, and sometimes blood count can be reviewed.
Falls risk, hearing, vision, bone risk, heart risk, cancer screening intervals, medicines, kidney function, alcohol effects, and independence planning.
Testing should reflect health, life expectancy, goals, frailty, prior screening, and whether a result would change treatment.
Sources
Use public guideline bodies for what to do in ordinary care, cancer agencies for patient-facing explanations, and journals or Cochrane when you want to understand the evidence fight underneath the recommendation.